

“Surgery can cure Type 2 diabetes”. This is a statement that would have sparked disbelief a few years ago – but it is now a reality.
For the first time in the treatment of diabetes, the discussion has moved beyond just ‘control’ to complete resolution. There are now a number of studies that have shown that a gastric bypass procedure results in remission of type 2 diabetes in around 70% of patients.
Research in patients who are undergoing surgery for obesity (bariatric surgery) has revealed some startling facts:
- Bariatric operations, such as gastric bypass and duodenal switch, have a profound effect on how glucose is metabolised (processed in the body), which is independent of weight loss due to the surgery
- Nearly all the procedures performed – gastric banding, gastric bypass, sleeve gastrectomy and duodenal switch to name a few – have marked effects on glucose metabolism
Whilst with gastric bands the resolution of diabetes is weight dependant and parallels the weight loss, with the other procedures, such a gastric bypass and sleeve gastrectomy, diabetes resolution occurs independent of weight loss due to the effects of these procedures on metabolism.
This resolution is more persistent in patients who have a shorter duration of Type 2 diabetes. In other words, surgery is more likely to result in long-term remission if it is performed early after diagnosis.
Evidence from clinical trials
There have been at least two trials performed in patients with diabetes undergoing surgery that have clearly demonstrated the short and long-term benefits of these procedures, as compared to best medical treatment. The STAMPEDE trial has demonstrated that up to a third of patients have resolution of diabetes 3 years after surgery compared to best medical care. This was seen with both the gastric bypass and sleeve gastrectomy.
It is based on such evidence that the American Diabetes Association (ADA) has recommended surgery as a treatment modality of Type 2 diabetes. It is also the rationale behind the National Institute of Clinical Excellence (NICE) recent recommendations for bariatric surgery. The criteria for surgery have been modified to include patients even with a BMI of 30-35 who have been recently diagnosed (less than 2 years) with Type 2 diabetes.
By what mechanism does the surgery resolve Type 2 diabetes?
Gastric bypass (see figure below) reduces the use of diabetes medications (both oral hypoglycaemic agents and insulin) in a weight-independent manner, and this is evident within days of the surgery (see case study at the end of this article).
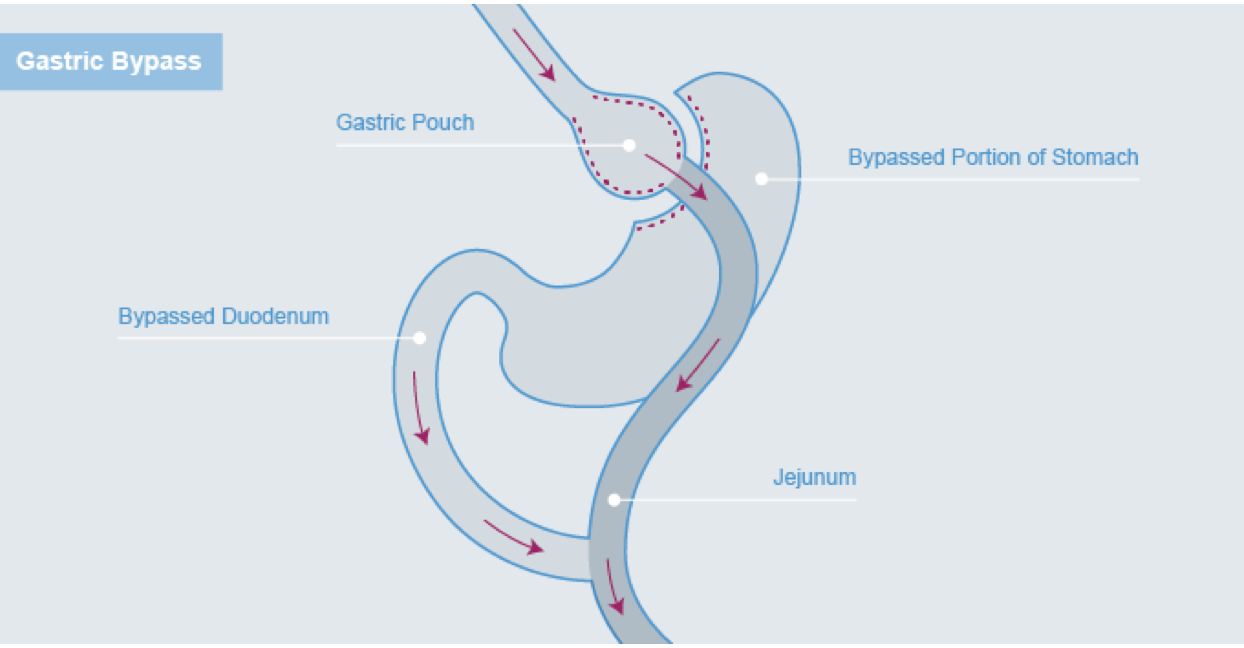
The exact neuro-humoral mechanisms behind these startling facts are currently being unravelled through some ground-breaking research.
The gastro-intestinal tract is one of the largest and most complex endocrine organs in the human body. Glucose homeostasis is maintained through a delicate balance between a group of gut hormones called incretins and anti-incretins. One of the best understood of these is Glucagon–Like Peptide-1 (GLP-1). Released by the small intestine in response to food, this hormone causes an increase in insulin levels and therefore lowering of blood glucose levels. In addition, there are at least five other gut hormones that play a critical role in glucose homeostasis. Bypassing the small intestine through surgery results in a profound effect on the release of these hormones and their resulting effect on blood sugar levels.
Case study
LM (name changed) is a 45–year mother of two who had been diagnosed with Type 2 diabetes 6 years ago. Her BMI was 37 (92 kg). She had tried losing weight through diet and exercise for over 10 years. Her diabetes was getting increasingly difficult to control and she came to see Mr Moorthy for consideration of surgery. Before being referred for surgery, she was on metformin 750 mg twice daily, and had just been started on 10 units of long–acting insulin a day.
She met the dietician and psychologist as part of the pre-operative counselling process and decided that a laparoscopic gastric bypass was in her best interest. She underwent the procedure and was started on a sliding scale (subcutaneous administrations of insulin depending on the blood glucose level) in the immediate post-operative period. As a result of her insulin requirement in the 72 hours following her surgery, she was discharged on only metformin 1 g twice daily.
She monitored her blood glucose level everyday, which she communicated to her metabolic physician through text messages, and was asked to stop all insulin injections 4 weeks after surgery.
She suffered no post-operative complications or problems and 6 months following her surgery she had lost 32 kgs and was on no medications for diabetes.
This article is for information only and should not be used for the diagnosis or treatment of medical conditions. myHealthSpecialist makes no representations as to the accuracy or completeness of any of the information in this article, or found by following any link from this article. Please consult a doctor or other healthcare professional for medical advice.

Mr Krishna Moorthy
Consultant Obesity and Upper-GI Surgeon