

Over the winter, many snowboarders, and to a lesser extent skiers, will unfortunately return from the slopes with a significant wrist injury. As snowboarding has become more popular, the incidence of such injuries has increased.
Snowboarders have both their feet strapped to the board, meaning that when they fall, they have a greater tendency to break that fall by putting out their hands. It is therefore important that those new to the sport are taught how to fall safely – either by rolling backwards onto their buttocks and back, or forwards onto their knees and forearms. There are also wrist guards available which reduce the chance of serious injury. Longer guards that extend some way up the forearm are to be recommended over shorter guards that end just above the wrist.
Types of wrist injuries
When falls occur at speed during skiing or snowboarding, two main structures in the wrist are most at risk:
- The distal end of the radius bone
- The scaphoid bone – a small bone within the wrist
Distal radius fractures
Usually, the force required to cause fractures to the distal end of the radius, particularly in younger patients with strong bone, is high – meaning that fractures often have more complex patterns than the fractures sustained by older patients in lower-energy falls. X-rays will demonstrate the fracture, but CT scanning is helpful in planning surgery for complex fractures.

Distal end of radius fractures
Scaphoid fractures
Fractures of the scaphoid are sometimes difficult to diagnose, and do not always heal well. The diagnosis is suspected if there is pain and tenderness in the “anatomical snuff box” of the wrist, but X-rays soon after the injury can be normal. MRI scanning is the most sensitive way of detecting a fracture that has not been seen on an X-ray.
Other injuries
Other injuries can of course occur, including ruptures of the small ligaments within the wrist. MRI scanning can be very helpful in demonstrating ligament injuries, although an arthroscopy (inspecting the inside of the wrist joint using a small telescope) is said to represent the gold standard.
Many other structures in the wrist and hand can be injured by falls on the slopes, including the small ligaments between the wrist bones, and the ulnar collateral ligament of the thumb (known as “skier’s thumb”). However the injuries mentioned above are the most common in snowboarders.
Management of wrist injuries
Distal radius fractures
Fractures of the distal radius that are not very ‘displaced’ can be well treated by applying a cast below the elbow, and maintaining it for 5-6 weeks. A period of physiotherapy will be required once the cast is removed to regain both range of motion and strength.
Displaced fractures are usually manipulated under anaesthetic or sedation into a better position, when the patient is first seen in an accident department. Definitive surgical treatment can then be planned, and will be required if the manipulation is only partially successful, if the joint surface is severely affected, or if the fracture re-displaces in the initial cast.
There are many ways to surgically restore the position of the fragments, and stabilise them while the fracture heals. In the majority of cases, specialist wrist surgeons will use a form of plate and screws specifically designed to be fixed to the palmar aspect of the bone, through an incision of around three inches:
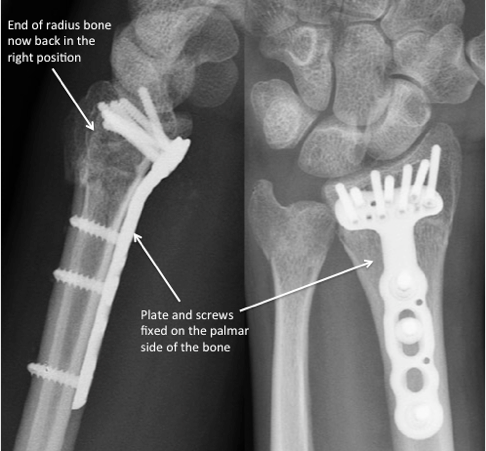
Plate and screws fixed to the palmar aspect of the bone
The advantages of this form of fixation are:
- Stability of the fracture site while it heals
- No need for further surgery – the plate can almost always be left in place
- Early rehabilitation – patients can start exercises within the first week of surgery, under the guidance of a hand therapist
- Earlier recovery of strength and range of motion than with more traditional techniques
- Can be used for treatment of complex fractures
Scaphoid fractures
Fractures of the far end of the scaphoid, towards the thumb, and some fractures of the mid-portion (‘waist’) of the scaphoid are usually well treated in a cast, but may need 8, or even 12, weeks to heal. Fractures of the near end of the scaphoid, and displaced fractures of the waist, do not heal so well.
Patients with these injuries may be offered a minimally-invasive operation (called “percutaneous fixation” or “mini-open fixation”) depending on the exact position of the fracture. A special type of screw is buried within the bone and effectively compresses the fracture site, encouraging fracture repair. This again has the advantage of reducing the time it is necessary to wear a cast, as well as increasing the likelihood of healing. Patients with undisplaced fractures can also choose to have this procedure carried out if they want to avoid the 8-12 weeks of limited mobility that wearing a cast brings.
Key points
- Snowboarders should learn how to fall safely, and should wear wrist guards to avoid serious wrist injury
- The distal end of the radius and the scaphoid bone are most at risk from a fall whilst snowboarding
- Specialised plates placed on the palmar aspect of the radius are used to allow early rehabilitation of the wrist after distal radius fracture
- Scaphoid fractures can be treated with minimally-invasive surgical fixation to increase the chance of healing and avoid prolonged cast immobilization

Mr Sam Gidwani, Consultant Hand and Wrist Surgeon
Book an appointment with Mr Sam Gidwani
www.londonhandsurgeon.co.uk